
Medpage Today reports that “a paper advocating against affirmative action in cardiology programs is melting under a blast of Twitter heat.”
Melting is more wishful thinking than reporting—the substance of the paper was untouched by the firestorm, which was instead inflamed by the author’s opinions—but the assault has indeed been vicious. It also raises an ominous warning: the combination of cancel culture and anti-racism threatens to turn the future of debate over race and affirmative action into no debate at all. Cancelers do not attempt to refute those they scorn; they attempt to silence them, often to great success.
“Rise up, colleagues!” tweeted Dr. Sharonne Hayes, Director of Diversity and Inclusion at the Mayo Clinic in Rochester, Minnesota. “The fact that this is published in ‘our’ journal should both enrage & activate all of us.” It did.
“We definitely need to address this,” tweeted Dr. Seyi Bolorunduro, a cardiologist in northern Virginia. “Unfortunately due to arguments like this, minority trainees are told that no matter how hard they work, they only occupy that position bcos of affirmative action.”
McMaster University cardiologist Dr. Harriette Van Spall tweeted that the article’s “historic stereotypes [don’t] account for structural biases that kids face leading up to their applications,” and, in another tweet, she called the article “incompatible with AHA [American Heart Association] values. We must,” she added, “examine mindsets + composition of those we empower with Ed board positions.”
A common theme of the complaints is that the article should not have been published. “How did this paper get past the reviewers and editors?” asked Duke University cardiologist Pamela Douglas, former president of the American College of Cardiology.
AHA officials and journal editors could not apologize fast enough. “I want to be very clear,” insisted Dr. Robert Harrington of Stanford, immediate past president of the American Heart Association, “that this paper is not at all aligned with our values as an organization.” Quoted in an article, “AHA, Editors, and Cardiologists Ask: How Did ‘Racist’ Paper Make It to Print?” Dr. Harrington told tctMD that the article never should have been published, that it is “pure opinion, an opinion that is really, really disturbing and distasteful.” It’s very important, he continued, “as we think of things like health equity to have a workforce that looks like the population we’re being asked to care for.” Wherever “equity” appears, proportional representation is never far behind.
Dr. Donald Lloyd-Jones, AHA president-elect, expressed his agreement shortly thereafter. “We look forward,” he tweeted, “to understanding how Dr Wang’s views, which do not represent AHA’s core values at all, could have been published given the unbalanced, unscientific, and untrue statements made, as well as the deeply concerning and hurtful opinions expressed.”
Dr. Barry London, Director of Cardiovascular Medicine at the University of Iowa Carver College of Medicine and editor-in-chief of the Journal of the American Heart Association, which published the offending article, quickly attached an abject apology to the site of the paper. “I apologize for my role and for the role of my staff in the publication of this viewpoint article,” he wrote. “JAHA will support all efforts to correct this error, including but not limited to the publication of alternate viewpoints, which we solicited at the time of publication but have not yet been submitted to the journal. In addition, we will work to improve our peer review system to prevent future missteps of this type.”
So, What’s All The Fuss About?
The target of this revealing, all-hands-on-deck assault is a seemingly anodyne, scholarly paper in the Journal of the American Heart Association, “Diversity, Inclusion, and Equity: Evolution of Race and Ethnicity Considerations for the Cardiology Workforce in the United States of America From 1969 to 2019,” by Professor Norman C. Wang of the University of Pittsburgh Medical School.
Anyone coming across this paper unaware of the firestorm of hyperventilation (verging on virtual coronaries) it provoked among woke cardiologists would be surprised to learn it had caused such an uproar. And that is especially true of anyone familiar with the by now extensive scholarly literature of and legal commentary on affirmative action. The paper’s approximately 12,000 words, with graphs, charts, and over 100 citations, although clearly written by a physician and not by a historian, lawyer, or even social scientist, is well-grounded in that scholarship and will surprise no one familiar with the field.
Wang presents a thorough history of the efforts of various medical associations to, first, encourage, and later to require increasing the number of blacks and Hispanics in medical school and the medical workforce. Some of these efforts will be unfamiliar, even to many who are acquainted with this general history, and thus I encourage all who follow the debate over affirmative action to put the tweets aside and read the whole paper.
Wang concludes that these attempts to approximate or even achieve proportional representation failed, as they were bound to, primarily because of “the limited qualified applicant pool.” Along the way he provides additional evidence to support Richard Sander’s and Stuart Taylor’s “mismatch” argument.
In addition, although his occasional legal arguments could have been stronger, Wang’s view that many of these efforts were illegal is clearly within the mainstream of those who criticize racial preference policies, such as Justice Thomas’s assertion in his Grutter dissent, which Wang quotes, that “the Law School tantalizes unprepared students with the promise of a University of Michigan degree and all of the opportunities that it offers. These overmatched students take the bait, only to find that they cannot succeed in the cauldron of competition. … And the aestheticists will never address the real problem facing ‘underrepresented minorities,’ instead continuing their social experiments on other people’s children.” No doubt equally infuriating to Wang’s critics was his quoting Justice Powell’s warning in Bakke that “preferential programs may only reinforce common stereotypes holding that certain groups are unable to achieve success without special protection based on a factor having no relationship to individual worth.”
According to tctMD, on August 6, just a few days after the article came under fire, the University of Pittsburgh Medical Center “notified the journal that the article ‘contains many misconceptions and misquotes and that together those inaccuracies, misstatements, and selective misreading of source materials strip the paper of its scientific validity.’ Following that, JAHA retracted the article.”
Not only was his article retracted, but one suspects that Wang himself would have been retracted if he did not have tenure (which I assume, as an associate professor, he has). Dr. Kathryn Berlacher, head of Pitt’s general cardiology fellowship, tweeted that Wang “was removed as EP PD (Electrophysiology Program Director] as soon as this was known…. I am [Program Director] of general cardiology fellowship at Pitt [and] will say again: We stand united for diversity equity and inclusion. And denounce this individual’s racist beliefs and paper.”
His supposed many misquotes, misconceptions, misreadings, and inaccuracies were not specified, but it is clear that what inflamed Wang’s critics was not his handling of the evidence, but rather his opposition to racial preference programs. Indeed, as Dr. Samir Saba, Chief of Cardiology at Pitt, frankly admitted to Medpage Today, Wang’s “opinions are incompatible with the values of our training program.”
In sifting through the tweet storm and the articles about this controversy, I saw only two criticisms of Dr. Wang that were not based entirely on his opinions or “misconceptions.” Former AHA president and Stanford cardiologist Dr. Harrington stated to tctMD that “Wang argues that while patients might feel more engaged and communicate better with doctors of the same race and ethnicity, ‘there exists no empirical evidence by accepted standards for causal inference to support the mantra that ‘diversity saves lives.’” That’s “simply not true,” Harrington asserted, referring to research at Stanford purporting to show that “Black patients were more likely to talk about their health problems and to engage with available preventive cardiovascular screening if they had a Black physician. That study suggested that Black doctors could lower reduce [sic] the number of deaths from cardiovascular disease and close the gap in cardiovascular mortality between white and Black men.”
Wang’s paper agreed with Harrington’s point about patient-to-doctor conversation, but it has much more than a mere assertion that diversity doesn’t save lives. It has an entire section devoted to the question, aptly titled “Does Diversity Save Lives?” He finds no persuasive evidence that it does. Dr. Harrington disagrees. Normally this debate would be carried on through competing peer-reviewed studies, but here Dr. Harrington and his allies attempt to eliminate Dr. Wang’s paper and remove him from the debate altogether.
Dr. Ann Marie Navar, a Ph.D. and M.D. at Duke, also attempted through nine tweets to offer some substantive criticisms, along with the conventional outrage—from tweet 1: “Shocking these statements are made by the director of the EP fellowship. … How does he evaluate Black/Hispanic applicants?” Either she doesn’t believe the obvious answer—on the basis of their qualifications—or she doesn’t think qualifications alone are sufficient.
Tweet 2: “Many refs he cites actually argue for more not less affirmative action.” True, but Navar, despite her double degrees, misreads Wang’s purpose in the citation she cites (his note 22). That publication does indeed advocate more affirmative action, but Wang cites it to support his view, which it does, “that progress had been attained only by lowering admissions standards for objective academic achievements.”
Tweet 3: “Older data cited on affirmative action leading to ‘unqualified’ people being admitted are confounded. Differential promotion and graduation rates between minority and white students likely attributable to institutional racism and differential resourcing.” Her use of “confounded” here confounds me.
It’s downhill from there. Tweet 5 says Wang “trivializes” by using quotation marks around “underrepresented” when writing that blacks and Hispanics are underrepresented in medicine. On the contrary, he doesn’t trivialize it; he simply opposes proportional representation. Tweet 6 claims that “Arguments that efforts to increase diversity hurt Asian colleagues not backed by much fact.” Really? Perhaps Dr./Dr. Navar is unfamiliar with the SFFA v. Harvard case.
In short, other than the above pathetic efforts by Drs. Harrington and Navar, the cardiologists’ conniptions were provoked by Dr. Wang solely on the basis of his opinions that do not “reflect,” or are not “compatible with,” the American Heart Association’s, the Journal of the American Heart Association’s, or the Pitt medical school’s “core values.”
Based on my reading of their attacks on Dr. Wang, I strongly suspect that the reason they concentrated on his opinions is that, despite their heavy involvement with engineering medical diversity, they are unfamiliar with the scholarship on which Dr. Wang drew and to which his article makes a significant contribution. How many of them, I wonder, have read Mismatch by Sander and Taylor, or are even familiar with its argument and the evidence supporting it?
What, then, are Dr. Wang’s opinions that are so vile that he and all the publications he rode in on should be canceled? We’ve seen that he believes “mismatch” is a real, provable problem and that he opposes proportional representation. What else? Here’s one from Dr. Wang’s conclusion that got the cardiologists’ blood boiling:
“Long‐term academic solutions and excellence should not be sacrificed for short‐term demographic optics.”
Another opinion, from the close of the article, reads: “We will have succeeded when we no longer think we require black doctors for black patients, chicano doctors for chicano patients, or gay doctors for gay patients, but rather good doctors for all patients. Evolution to strategies that are neutral to race and ethnicity is essential. Ultimately, all who aspire to a profession in medicine and cardiology must be assessed as individuals on the basis of their personal merits, not their racial and ethnic identities.”
Hans Bader makes a powerful argument in Liberty Unyielding, citing chapter and verse from a number of cases, that Prof. Wang’s academic freedom and First Amendment rights have been trampled. Roger Clegg adds, incisively, “that it’s reprehensible to punish people for telling the truth, whatever the law allows.” And I am tempted to add that the deeper tragedy here is what the treatment of Dr. Wang reveals about the sorry state of discourse over controversial issues, especially involving race. But in fact, it’s worse than that. Because of such responses as the ones here by the woke, there cannot even be any discourse. How, for example, can there be a debate on the pending Proposition 16 in California, which if passed would remove the state’s prohibition against preferential treatment, when opposing it by saying the sort of things Dr. Wang said is likely to get you fired, or worse?
Far too little appreciated is how great the ever-widening gulf is between the woke elitists in academia and what, for now at least, remains mainstream American opinion. Gallup provided new evidence of what the mainstream still believes only a few days ago: on August 7, Frank Newport, a Gallup senior scientist, published a timely review of American opinion on affirmative action “in the context of Black Lives Matter and the renewed societal emphasis on discrimination.”
Newport reviewed a number of polls confirming that, if you ask respondents a “question about affirmative action without a definition or explanation, e.g. ‘Do you generally favor or oppose affirmative action programs for racial minorities?’,” about 60% will say they support it. But when the question includes a description of how affirmative action actually works—that is, do they support “policies that explicitly take race into account to achieve these objectives”—the results are more than reversed.
For example, he linked to a 2019 Pew Foundation poll that asked, “When it comes to decisions about hiring and promotions, do you think companies and organizations should take a person’s race and ethnicity into account, in addition to their qualifications, in order to increase diversity in the workplace (or) should only take a person’s qualifications into account, even if it results in less diversity in the workplace?” 74% opposed taking race into account.
Similarly, he pointed to a question last asked by the General Social Survey in 2018: “Some people say that because of past discrimination, blacks should be given preference in hiring and promotion. Others say that such preference in hiring and promotion of blacks is wrong because it discriminates against whites. What about your opinion — are you for or against preferential hiring and promotion of blacks?” 72% opposed preferential treatment for blacks, including 43% who say they oppose strongly.
Perhaps academic cardiologists were not adequately represented among the respondents.
The last word goes to someone who replied to Dr. Navar’s tweets discussed above by supplying this chart from the Association of Medical Colleges, which shows the acceptance rates of applicants by race in different bands of GPAs and MCAT scores:
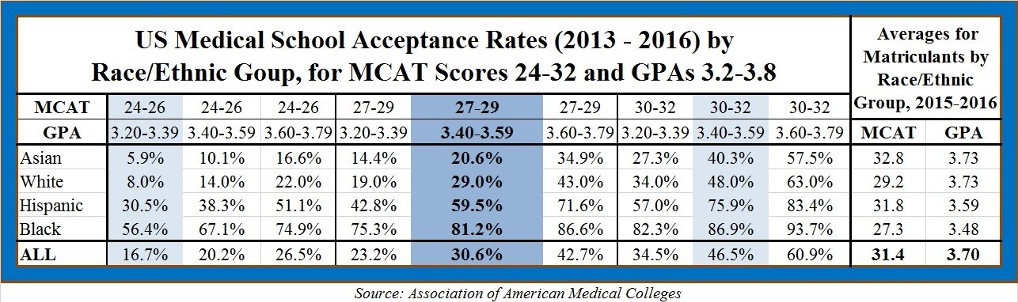
He asked, “Do you possess a conscience? Or are you so blinkered by your ideological tunnel vision that you can read these stats without disgust.” He concluded with a modest proposal: “Existing discrimination against Asians and whites in medical school admissions isn’t enough. May I suggest we ramp it up even higher? Isn’t that what Anti-Racism demands?”
Yes, it is. Just ask best-selling anti-racism guru Ibram X. Kendi, who asserts here that “racial discrimination is the sole cause of racial disparities” and here that:
If discrimination is creating equity, then it is antiracist. If discrimination is creating inequity, then it is racist. . . . The only remedy to racist discrimination is antiracist discrimination. The only remedy to past discrimination is present discrimination. The only remedy to present discrimination is future discrimination.
Do not disagree unless you want to be canceled.
Image: Crazypaco, Public Domain
{kind=link}
Between this and the politics of the Wuhan Virus, medicine risks losing the public respect which it currently enjoys. And if it loses that, it likely will also lose the disproportionate share of economic resources which it also currently enjoys.
I want a qualified cardiologist. Affirmative action makes me want a white or Asian, since they have a hurdle to overcome, their race.
Your view is very common. I’ve heard that black and hispanic doctors have a hard time getting patients (this necessarily includes black and hispanic patients, otherwise they would not have such trouble), while whites and Asians are overbooked, because the public assumes they are there because of affirmative action.
And statistically it is a good assumption. You’re not supposed to say it. But they can’t, so far, stop people from thinking it and acting on the thought.
The way to really get rid of this perception is to get rid of the fact. Assess people on skill-based qualification measures, period.
But the field has walked away from that, and they say it honestly. They say, clearly and loudly, that the following statement from the paper is incompatible with their values: “Ultimately, all who aspire to a profession in medicine and cardiology must be assessed as individuals on the basis of their personal merits, not their racial and ethnic identities.” So patients, including black and hispanic patients, will continue to try to make the adjustment themselves in their choice of doctor.
They’re going full Mao. Never go full Mao! I should know, my first overseas ESL teaching job was in Nanjing, People’s Republic of China, in 1987-1988. At the time, Deng Xiaoping’s economic reforms were just starting to kick in, so I was able to see firsthand everybody, and I mean everybody running in the opposite direction from the words of Karl and Mao.
I disagree, these programs are fundamentally in-egalitarian unlike Mao’s, who still actually enjoys considerable popularity in China, while affirmative action enjoys practically no support among working-class Whites in America.
“he only remedy to racist discrimination is antiracist discrimination. The only remedy to past discrimination is present discrimination. The only remedy to present discrimination is future discrimination.” – Ibram X. Kendi
Shorter version:
“Segregation now, segregation tomorrow and segregation forever.” – George Wallace
Thank you! Well written!
Horrifying. We are entering a new dark age, from which we may not emerge.
Thanks for this article. One complaint, though, if I might offer it – the replacement of “black” with “Black,” is one politically correct move that needs to be resisted – especially if it is paired with “white” instead of “White.” It is bad enough if both are capitalized.
It’s a new trick of the Left’s and has to be fought before it becomes entrenched. Thanks.
These woke cardiologists need to be asked just one question: would you be okay knowing the surgeon about to perform open-heart surgery on your child was an affirmative action admit to medical school?
They would say one thing and do another, guaranteed.